 At a meeting of the Glasgow Pathological and Clinical Society on November 13th 1877, members had a rare treat. The British Medical Journal for the following month takes up the story:
At a meeting of the Glasgow Pathological and Clinical Society on November 13th 1877, members had a rare treat. The British Medical Journal for the following month takes up the story:
Dr. David Foulis showed the parts removed by him in the operation of excision of the larynx, viz.: the cricoid and thyroid cartilages.
The thyroid cartilage is the structure surrounding the trachea which makes up the Adam’s apple; the cricoid cartilage is just below it.
 The patient came under his care, in the Throat Dispensary, in May 1876.
The patient came under his care, in the Throat Dispensary, in May 1876.
A contemporary newspaper report identifies the patient as ‘James Houston, a cloth worker, twenty-nine years of age, a native of Campsea, near Glasgow.’
At that time, there was a small growth on the underside of the anterior end of the left vocal cord. The symptoms were hoarseness, inability to shout, and occasional sudden interruption of the voice in the middle of a word. Dr. George Buchanan kindly admitted the patient into his wards, and removed the growth by cricotomy, a small vertical incision in the skin, one inch and a half in length, exposing the region sufficiently for the purpose.
A cricotomy (an archaic term, as far as I can establish) is simply an incision into the cricoid. This was not itself a treatment, but allowed the surgeon access to the vocal cords in order to cut out the growth.
A year after the operation, the tumour had reappeared, and had assumed such a size as to again necessitate removal. Dr. Foulis, therefore, had the patient admitted into the Training Home for Nurses and performed thyrotomy, splitting the thyroid cartilage vertically in the middle line, holding the two halves apart with hooks, and clipping out the tumour, the seat of which was then touched with the actual cautery.
By cauterising it with hot metal, Dr Foulis hoped to kill the malignant tissue. Caustic agents were sometimes used for the same purpose.
The patient made a good recovery; but, six months later, the growth had reappeared in a more rapidly growing form. It was decided not to again attempt mere excision of the growth, and Dr. Foulis proposed the removal of the whole larynx with the tumour, to which the patient agreed.
A brave decision, but probably the patient’s only hope. Surgical removal of the larynx – known as laryngectomy – was a new and hazardous operation that had only been accomplished a few times before. The first to do so was Theodor Billroth, a great surgeon respected throughout Europe. On December 31st 1873 he operated on a patient who, like James Houston, had a rapidly growing cancer of the vocal cords. The operation (under chloroform anaesthesia) took an hour and three quarters, and was ‘frequently interrupted by strong coughing spells during which blood in rather large amounts was expelled via the trachea.’ Some time after the patient had recovered, Billroth fitted him with an artificial larynx. Dr Foulis had followed these developments with great interest; now he had the chance to perform the operation himself.
On September 10th, 1877, Dr. Foulis excised the larynx. He made a single vertical incision from the hyoid bone to the second ring of the trachea. The soft tissues were then carefully dissected off from the thyroid cartilage, first on one side and then on the other, leaving the larynx attached behind and at the lower and upper ends only. The lower end was then cut across; a large curved tube was put into the trachea…
To maintain an airway while the rest of the operation was in progress; otherwise blood and other unwanted substances might find their way to the lungs.
…and the laryngeal box was dissected cleanly away from its attachments behind and above. The patient made a good recovery, being able to swallow porridge and milk on the twelfth day after the operation, and to dispense with artificial feeding on the fifteenth day.
Billroth’s first patient was fortunate to escape infection; luckily, so did James Houston.
As soon as the wound contracted sufficiently, a vulcanite laryngeal tube was fitted in, and, by means of a simple arrangement, a vibrating reed was introduced, which took the place of the vocal cord.
Vulcanite (now generally known as ebonite) is a particularly hard type of vulcanised rubber. Its applications were similar to those of Bakelite and other early polymers in later decades.
Dr. Foulis showed the patient, and the method of applying and removing the tubes. The patient spoke in a resonant, loud, and clear but monotonous voice, repeating the names of the members of the Society, fragments of the English church-service, and finally all the vowel-sounds, with the greatest clearness and ease.
One newspaper reported that ‘he read passages from the prayer book’.
The reed was then removed, and the patient whispered the vowel sounds in a voice which was audible all over the room, proving that the vowel-sounds are produced by the modification of the oral and pharyngeal cavity, and not by variations in the vocal cords.
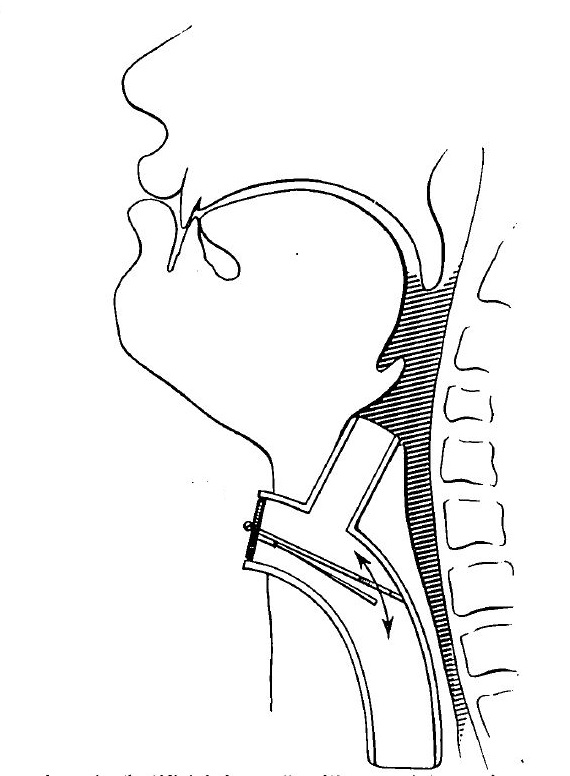
The artificial larynx was a simple device, effectively a length of tubing connecting the trachea with the back of the throat. In the middle was a single reed which vibrated when air passed over it, much like the reed of a clarinet. Foulis’s version was an improvement of the device used by Billroth three years earlier.
Those fusty old dullards at the British Medical Journal missed out the best bit of the whole story, however. As reported in The Times:
The reeds are made of metal, vulcanite, ivory, horn, etc., and the patient himself is fond of making reeds which give his voice new and surprising tones.
Now that’s what I call a hobby.
Pingback: Whewell’s Gazette: Year 03, Vol. #41 | Whewell's Ghost