One of the most famous of all medical marvels is the case of Phineas Gage, the American railroad worker who somehow survived having a large metal rod driven straight through his head. It’s a truly amazing story, but has been written about so often that you might be led to think that it was the only interesting thing to happen to an American doctor in the nineteenth century.
Less than a decade after Gage suffered his terrible accident, a case report almost as extraordinary – and with some uncanny parallels – appeared in the Atlanta Medical and Surgical Journal. The author was Dr William Rutherford from Harrisburg, Pennsylvania, and his article was published in October 1857.

On the morning of the 23rd July, about three o’clock, I was requested to visit Mr. Edward Thomas, at Highspire, a village on the Pennsylvania Canal, six miles east of Harrisburg, who was said to be seriously injured by his head striking against a canal bridge whilst asleep on the deck of his boat. I reached Hillspire about 4.30, and found Mr. Thomas in bed, his hair filled and matted with blood, his vest, shirt, upper part of his pantaloons and bed saturated with it, and a horrible looking rent in the scalp from the right superciliary ridge to the occipital bone.
Imagine a laceration stretching from the right eyebrow to the back of the head. This was a really dreadful injury.
The wound was filled with coagulated blood, which stood up high above the level of the surrounding parts, and some blood still oozed from the wound. In a cloth, on a bench on the opposite side of the cabin…
Before reading on, try to guess what object the doctor found ‘in a cloth, on a bench on the opposite side of the cabin’. Ready?
…was rolled up a portion of the malar bone, some fragments of the os frontis, and the entire right parietal, detached from its fellow along the sagittal suture, and from the occipital along the lambdoidal suture, or perhaps taking some part of the occipital bone with it, together with the squamous portion of the temporal bone.
Yes, the doctor found part of the patient’s skull lying on a bench. And not a small part, either. This was a huge bone fragment, measuring seven inches by six (18 cm x 15 cm), consisting of much of the right side of the skull, approximately between the top of the ear and the crown of the head. At a much later date it was photographed, and the image gives some idea of its sheer size – although one has to bear in mind that the photo does not include a number of other smaller bone fragments which were not preserved.
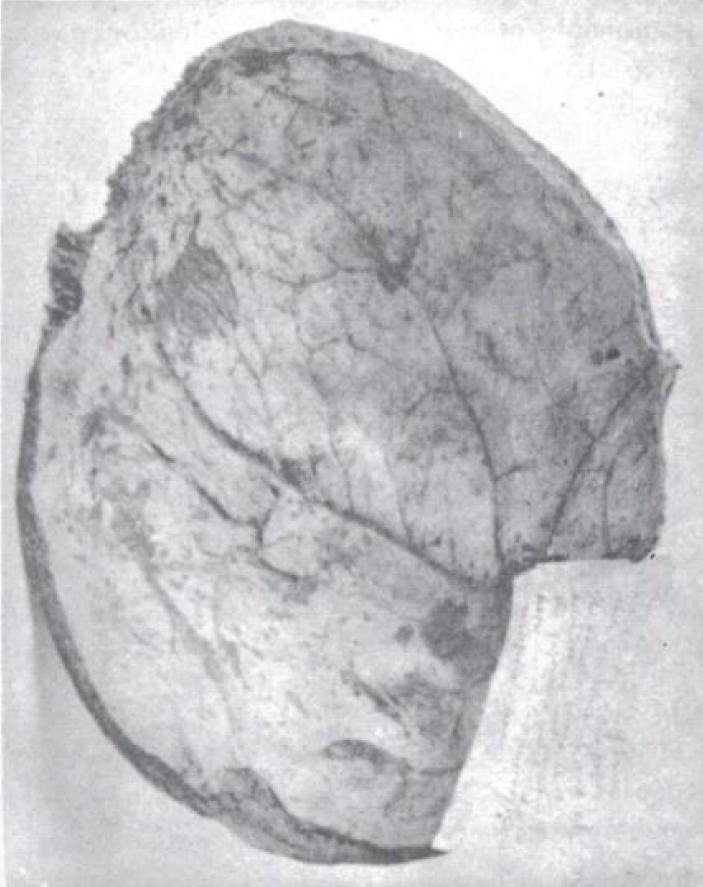
It was as clear of soft parts as if it had been removed from the dead subject with scalpel and saw.
A telling detail. The mechanism of injury in this case must have been exceptional for the scalp and skull to have been removed so incredibly cleanly.
His pulse was small, moderately frequent, and rather feeble; skin rather below the natural temperature, but not much. Said he did not suffer much pain. His mind was perfectly undisturbed, quick and vigorous. I asked him if the sight of the right eye was impaired; he closed the left with his hand and said the vision of the right eye was perfect.
The reason for this test: the patient had lost much of the zygomatic (malar) bone which forms part of the eye socket. With part of the eye’s bony support missing it’s surprising that his vision was unaffected.
He had no feeling of faintness, sickness of stomach, or any symptoms of concussion of the brain. The diminished force and volume and increased frequency of the pulse were, I think, owing entirely to the loss of blood.
Which sounds plausible.
I suggested to Dr Putt, who was in attendance with me, that it would be very difficult to dress the wound in the position in which Mr Thomas was then lying. Mr. Thomas said he would sit up, and immediately got up and seated himself on a chair in the middle of the cabin floor.
“Tell you what, Mr Thomas, since you’ve lost much of your skull and possibly some of your brain tissue as well, why don’t you just keep lying there and let us worry about how to dress the wound?” is what a doctor probably ought to say in this situation.
We removed the hair an inch and a half or two inches from each side of the wound with scissors, and then shaved the scalp with a razor. I then examined the wound with my finger, and found two loose pieces of bone about the superciliary ridge, which I removed. I then took a pocket-case spatula and commenced at the posterior angle of the wound, and removed a sufficiency of the coagulum to allow the edges of the scalp to be brought together by suture, then proceeded to remove some more and introduced another stitch, &c., until I had the wound in its whole extent very nearly brought together.
For a doctor in 1857, confronted by such a catastrophic injury, it must have been difficult to know what to do. So Dr Rutherford did the basics: clean the wound and attempt to stitch it up. Today a surgeon might possibly try to clean up the skull fragment and replace it – if it still looked viable – but that was hardly an option in the pre-antiseptic era.
In the clots which I removed I did not discover any discharged brain, nor did I get a sight of the membranes of the brain, for I was apprehensive if I removed the coagulated blood entirely that fresh haemorrhage would ensue. Indeed I concluded the less the brain was meddled with in that unprotected state the better.
Sensible advice!
The dressing occupied an hour or more, at the end of which he rose to his feet and removed his vest and shirt and put on a clean one; he then took off his pantaloons, and being handed a clean pair, poised himself on one foot and thrust the other into the leg of the pantaloons, changed feet, and thrust in the other leg, drew them up, buttoned and adjusted them with care, just as if nothing had happened to him, and walked over to his bed and laid himself down. He was not aware he had lost so much bone, or perhaps any, for it was concealed from him.
Horrifying. The patient’s brain was protected by little more than a thin layer of gauze, but he was still allowed to caper around his room and put himself to bed.
About 6 o’clock I left him after applying a wet towel to his head, and at ten o’clock saw him again in company of two of our Harrisburg physicians, as the boat passed through the locks at this place. Considerable reaction had occurred; his pulse was full, tolerably strong and about 80; skin warm, mind clear, but little pain, scarce any drowsiness, and his feelings he said quite comfortable.
‘Reaction’ is a piece of nineteenth-century medical jargon, essentially meaning ‘recovery’. A treatise on the treatment of wounds published in the 1880s explains that ‘when the vital powers rally from [the] state of depression and the different organs begin to resume their proper functions, reaction is said to have taken place.’
Since the accident, I have learned that it was produced by the end of one of the suspension rods which holds the string-pieces to the arch, the end of which projected below the timbers.
The mechanism of injury is intriguing. Judging by the soft tissue injury, the first point of impact was somewhere around the right eyebrow. Perhaps the suspension rod snagged the outer part of the right orbit – there is a weak spot in the skull at this point, the zygomaticofrontal suture. It then seems to have levered off a good chunk of the frontal, temporal and parietal bones in much the same way as an opener takes a cap off a beer bottle. The miracle is that it didn’t take much of Mr Thomas’s brain with it.
If it were not for the fact that two physicians of this place, and Dr Putt, of Highspire, have seen the patient, together with Dr Seaman’s letters, I should doubt the propriety of publishing it in a respectable medical journal, for really it is almost too marvellous for belief.
You’re telling me.
Here is a man with nearly half of his skull torn away without any cerebral disturbance whatever, indeed without any symptoms to indicate the injury he has received except the torn scalp and the haemorrhage. Thus I concluded a hasty but truthful statement of the case as it came under my observation.
The original case report was accompanied by three letters written by the patient’s brother-in-law Dr Seaman, updating Dr Rutherford on the patient’s condition. On July 30th, Dr Seaman writes:
My brother-in-law, Edward Thomas, the boat captain whose head was so seriously injured by a bridge with so much loss of the bony structure, which was dressed by you on the morning of the 23rd inst., near Harrisburg, requests me to write to you, and inform you that he is still living, and in full possession of all his mental faculties.
The patient had an excellent appetite, and his symptoms were relatively trivial.
Complains of some dull pain in the head, helps himself up with ease, but when he starts up suddenly, as he sometimes does, from sleep, there will take place immediately considerable haemorrhage from the wound. On the whole he is very comfortable and hopes are beginning to be entertained by his friends of his ultimate recovery.
Five days later came this update:
This is the thirteenth day since he received the injury, and strange as it may seem he is doing well. During the first ten days succeeding the wound, there was considerable and frequent returns of haemorrhage from it, which would occur on almost every effort to sit up or even turn over in bed, but was readily arrested, in most instances, by the more frequent application of ice water. Since suppuration has commenced the bleeding has ceased.
A week after the accident, Dr Seaman removed the surgical dressing. He had a shock.
The edges of the wound were widely parted, the scalp hanging in a fold over the ear, leaving a portion of the surface of the brain the length of the wound and one and one-half inch wide exposed to view.
The horror. The good doctor realised that he could not leave the patient in this situation, so he shaved the rest of the scalp and managed to bring the edges of the wound together using adhesive straps and a bandage.
Despite the upbeat tone of the letters, there is no doubt that the patient’s life hung in the balance. With nothing but skin protecting his brain, an otherwise trivial accident might have been fatal, and infection might have set in at any time.
The third and final update is dated August 8 1857. Dr Seaman reports that the patient ‘has been improving rapidly’:
He does not complain of as much pain in his head and ears as formerly, and sits up in a chair two or three hours per day. His appetite is good, rests well at night, and has been walking about the house this afternoon without much apparent fatigue. At present he is recovering very fast, and if no unfavorable change should take place, he will soon be quite well.
Dr Seaman suggests that the patient had lost ‘nearly one-half’ of his skull, which seems a somewhat generous estimate.
I had forgotten to mention above that his intellect remains undisturbed, that considerable of the lower portion of the right front lobe of the brain was so injured that it has sloughed away.
Interesting. Frontal lobe injuries, even quite severe ones, can have effects that may not immediately be obvious. Movement and sensation are typically unaffected, but the patient’s ability to express emotions, plan ahead or behave appropriately in a social situation may be impaired (among other things).
Dr Seaman concludes his final communication with the jaunty – flippant, even – suggestion that perhaps humans
do not require such cumbrous bony structures, filled with so much chaff called brains, as many of us carry on our shoulders.
There’s an astonishing postscript to this already amazing story. Two decades later a paper in the American Journal of Insanity reproduced the original case report, but with an update:
The man fully recovered, married a few months afterward, and is now the father of five children. He has maintained good general health, has never suffered from mental disturbance, and the only inconvenience he has experienced, has been a sense of fullness in the head when making active exertion or stooping over.
It was only 26 years after his accident that Edward Thomas started to suffer any serious effects. In 1883 he began to have difficulty walking, which developed slowly into left-sided paralysis. Four years later he was admitted to Buffalo General Hospital for treatment. The young doctor who treated him, William Bergtold, reported that in addition to suffering from left-sided hemiplegia, Thomas was displaying some classic symptoms of frontal lobe injury.
Patient presents no delusions, hallucinations, etc. He is, however, irritable and easily disturbed. Mental equilibrium readily destroyed. Sobs uncontrollably when criticised or a sup- posed slight or injustice has occurred to him.
Since the root cause of his illness was a catastrophic brain injury suffered almost thirty years earlier there was not much the hospital could offer in the way of treatment – except for a little electrical therapy, or ‘faradization’ as it was known then.
Beyond a general tonic and hygienic treatment nothing was done for him save faradization of the paralyzed parts. He left the hospital October 24, 1887, considerably improved; was able to go about easier, and could raise left forearm a few inches higher.
And that’s the last we know of Edward Thomas, the remarkable survivor of a remarkable accident. But thanks to this last report we can at least put a face to the name.