This blog has previously included a few cases in which a patient performed surgery on their own body. One of my favourites is the story of Colonel Martin, who found an ingenious way to reduce the size of a bladder stone, inserting a file up his own urethra to scrape it into submission.
That takes some beating, but in 1884 the Glasgow Medical Journal published a case which, while similar, was even more spectacular. The editor must have known it was a corker, since he gave it this none-too-modest headline:
The author of the article, Alexander Patterson, was a Glasgow surgeon, a colleague of the celebrated Joseph Lister and, in later years, a notable authority on kidney disease. It was not Dr Patterson who treated the patient in question, however, but a doctor identified only as ‘G.W.’:
J.B., a retired draper, was born in the year 1828, and in his youth was a factory operative. In 1845, when at the age of 17, he fell down the well of a hoist, alighting with his legs astride an iron bar, sustaining a double fracture of the left leg, also rupture of the urethra, and laceration of the perineum.
It sounds a horrible injury, but he would appear at least to have escaped with certain other prize assets intact.
Through the opening in the perineum, as well as by the urethra, blood passed for a period of two weeks.
He had suffered a perineal fistula, a wound in the space between the anus and scrotum.
Two attempts at closure of the perineal fistula were ineffectually made, and the urine continued to dribble without ceasing, compelling B. to resort to padding his clothing for the purpose of absorbing the constantly escaping urine. Several medical men saw him, but as the patient was much averse to any operative procedure, nothing was attempted, although the patient was aware from the year 1852 of the presence of a calculus.
A calculus being a stone in the bladder.
On the 14th June, 1872, Dr G.W. was called to see the patient, who was then complaining of pain in the bladder, for the relief of which sedatives were prescribed.
The following month the doctor visited again. The patient was sure he had a large bladder stone, and suggested that the physician insert his finger into the wound so that he could feel it for himself.
On passing his finger through the opening, the doctor at once felt the calculus, but his finger entered a large irregular cavity in the stone, and the patient explained the presence of this by saying that he had introduced a chisel, with which he attempted to break up the mass, and had managed in this way to remove about one ounce.
That’s right, folks: he had been trying to chip away a calculus from inside his own bladder. Using a chisel.
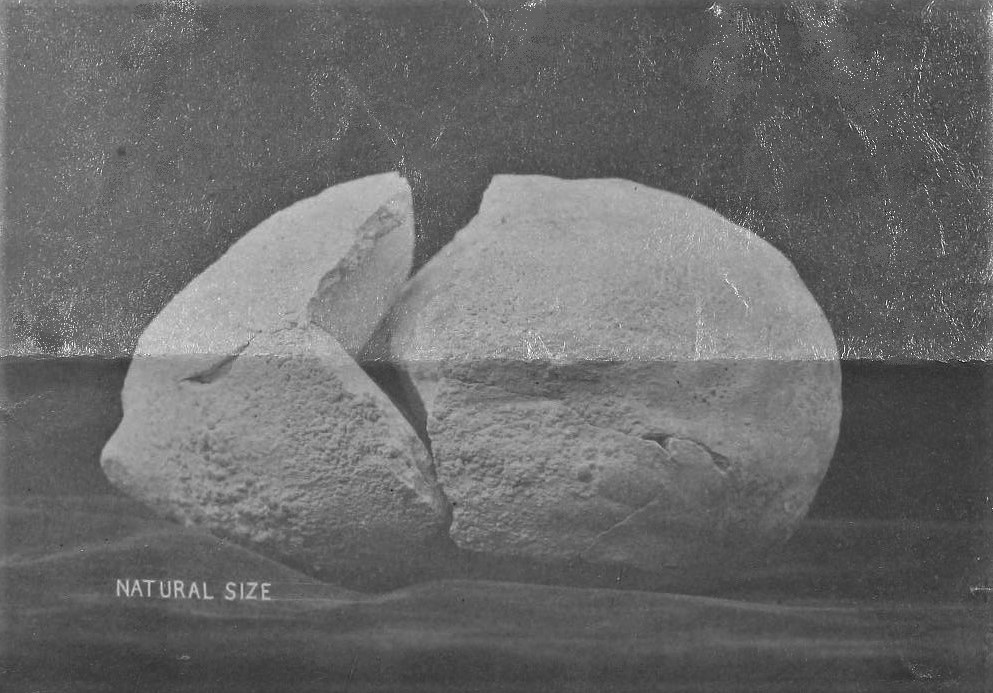
The doctor started home for forceps, with which to remove the stone, but during his absence, whilst B. was walking about his room in great pain, the stone suddenly burst the perineum, and fell heavily on the floor, breaking into two pieces.
Better out than in, as they say, but this event does not sound remotely enjoyable.
When expelled it weighed nearly 14 ounces and a half, which, taken with the portion removed by the chisel, makes 15 ounces and a half, which is, so far as I can discover, about the heaviest stone on record in the annals of surgery, in which the patient recovered after its removal. The stone measured in long circumference 10⅝ in., and in the short circumference 8⅛ inches.
At close to a pound in weight (450g) this was an enormous bladder stone, and at the time one of the largest on record. There have since been several well-documented cases of stones of 1 kg or more, with the current record-holder weighing in at a painful 1.9 kg.
But back to 1828 and the unfortunate J.B.:
The lacerated perineum was dressed with carbolic oil.
A recent innovation. The great Glasgow surgeon Joseph Lister had first started using carbolic acid (phenol) on wounds to prevent infection seven years earlier, reporting his experience in a famous series of articles for The Lancet in 1867. Alexander Patterson, the author of this case report, was among the first of his colleagues to adopt the antiseptic technique, and gave a talk on the subject to a local surgical society in 1873.
On the 15th July, six days from the date of expulsion of the stone, B. was going about collecting his rents and performing his other duties. During the last two years of his life Dr D. saw him occasionally. He passed his water with difficulty, and was fully convinced that there was another stone in his bladder.
The doctor tried to confirm this suspicion by passing an instrument into the bladder, but it proved impossible to insert even the slimmest catheter – perhaps because the stone had obstructed the top of the urethra.
The patient died in December, 1883, at the age of 55, of an apoplectic attack, eleven years after the passage of the stone.
An ‘apoplectic attack’ usually meant a stroke, an aneurysm or bleed into the brain.
Unusually for a journal of this date (1884), the article is illustrated by a photograph of the bladder stone, and you can clearly see where it broke when it fell out of the poor man’s bladder and on to the floor. It looks more like a dinosaur egg than a bladder stone – and probably felt like one, too.